WHAT DRIVES PATIENTS' CHOICE OF DESTINATION HOSPITALS – CURE, COST, OR COMFORT?
Zack Varughese, Ph.D., Professor of Healthcare Administration, OSU Center for Health Sciences,
Todd Arnold, Ph.D., Professor of Marketing in Spears School of Business, Oklahoma State University
Dursun Delen, Ph.D., Professor of Management Science and Information Systems, Oklahoma State University
Xiang Fang, Ph.D., Professor of Marketing in Spears School of Business, Oklahoma State University
Abstract
This study investigated the impact of built environment (i.e., "servicescape") on patients' choice of destination hospitals. It is widely known that factors such as hospital reputation, cost of treatment, and travel related concerns impact patients' choice of hospital, but little is known about the impact of servicescape on patients' hospital selection process. The findings, investigated within the context of cancer treatment, suggest that while reputation, cost, and distance are strong drivers in patients' choice, servicescape also impacts choice. Further, it is found that patients will travel long distance to choose a treatment center provided that it has a good reputation for high quality care and the "servicescape" is appropriate. The findings contribute to a deeper understanding of the relationship between consumer behavior and servicescape in a new dimension, the choice of cancer hospitals. The findings set the stage for additional research in this area. We believe these findings are valuable for both scholars and manager
Keywords:Patients' choice, destination hospital, reputation, cost, quality, medical tourism, distance, servicescape
1. INTRODUCTION
When faced with a sub-acute illness (e.g., back pain, pneumonia, or other relatively minor conditions), the majority of patients will choose a hospital near to home or one recommended by their physicians. But when struck with a terminal illness, the decision-making process becomes more complicated and several factors can impact the patient's choice of where to receive care. For example, Porell and Adams report that distance to a hospital is an important factor affecting hospital choice.1 Factors such as reputation, quality, and cost have been shown to impact patients' choices.2,3,4,5
With ever-increasing consumerism and a focus upon the "consumer journey", the trend towards health and healing has changed considerably in the last decade. The new trend is for patients to expect not only a cure but also an experience, derived from a combination of factors such as the location of the center, environment and ambiance, and customer service. Also, patients used to travel from developing to developed countries in search of better care. But it has changed recently: patients tend to travel from developed to developing countries.6 The motivation for such organized travel outside one's local environment is for quality, affordability, and comfort.7,8,9 With these new trends, and consistent with the idea of enhanced experience and journey, researchers have identified yet another factor that impacts health care choices -- servicescape.10
The term "servicescape" was first coined by Bitner to refer to the impact of physical surroundings on customer behavior.11 Her study's framework describes how the built environment (i.e., the man-made, physical surroundings as opposed to the natural or social environment) affects both consumers and employees in service organizations. Although scholars have devoted considerable effort to studying the factors that impact hospital choice, one thing that has received limited attention is the design of the service environment (servicescape) and its impact on hospital choice. Mari and Poggesi confirmed the above notion through a systematic study of servicescape, using 188 previous studies.12 Their study pointed out that much of the work on servicescape was done in retail settings and suggested including other service firms, such as banks and hospitals.
Rosenbaum and Massiah conducted research to expand on Bitner's work.13 They concur with Mari & Poggesi that most of the research tested servicescape in non-healthcare environments. 12From the studies of Rosenbaum and Massiah, and Mari and Pogessi, it is clear that the study of hospital choices incorporating all four key aspects - reputation, cost, distance, and servicescape- is still lacking.12,13 Thus, this study aims at filling the gap through a comprehensive study of the impact of reputation, cost, distance, and sevicescape on patient choice.
1.1 Importance of the Study
This study is important from the context of changes in the U.S. healthcare industry. The cost of healthcare in the U.S. has skyrocketed in the past decade, forcing U.S. customers to look into international treatment options, mostly in developing countries. Interestingly, these hospitals not only provide affordable, high-quality care, they combine comfort/pleasure with care, forcing U.S. hospitals to rethink the way they deliver care. These hospitals make every effort to provide treatment with a touch of class: hotel-like hospital buildings located in a resort-like settings; concierge service; state-of-the-art technology; and service delivered by a
highly talented,customer-oriented team.Therefore, this study is important in understanding the impact of servicescape on patients' choices of hospitals within a U.S. context.
Secondly,the study of servicescape is important from a theory development perspective. Among marketing academics, Bitner produced the seminal work on servicescape.11 Since Bitner's original model of servicescape, other variations of the model have evolved.11,12,13 However, retail settings were the most widely investigated.12 Therefore, Mari and Poggessi suggested extending the study to other service firms such as hotels, airports, hospitals.12 As only limited studies have incorporated the impact of servicescape in hospital design, this study will contribute to theory development in this area.
2. LITERATURE REVIEW AND THE DEVELOPMENT OF THE HYPOTHESES
In this section, we will start with an examination of different drivers of patients' choices of hospitals, followed by discussion of each driver and hypothesis development.
Lee et al. point out, how people choose is diverse and its influencing factors are very complicated.5 The medical care industry has dramatically changed over the last two decades in America. Providers and commercial payers have struggled to maintain quality, cost, and accessibility. The evolution of the internet and consumerism has also changed the way people choose hospitals. Lee at al. suggest that hospitals must therefore learn to respect consumers, develop distinguishing features of medical care, explore their needs, and improve satisfaction.5 Thus it is important to understand those factors that impact the relationship between consumers and hospitals. In this section, we will review factors that impact patient choice and hypothetical patient choice. To examine the different drivers of patients' choices of hospitals, we use the study of Lee et al. as it consists of a review of multiple studies in this area (Table 1).5 We reviewed other studies as well.8,11,12,13,14,15,16 Based on their relevance, we finally selected four major factors that impact patient choice: reputation, cost, distance, and servicescape, which we will examine in the following discussion. Key articles are shown in Table 1.

2.1 Reputation
One factor that consistently appears as being relevant in hospital choice is the reputation of the hospital.8,14,17 A hospital's reputation is based on its historical performance in terms of both quality and service. An institution's reputation may also be dependent upon the competency of its medical staff and endorsements received by accreditation and regulatory agencies.
Studies conducted in the U.S. point out that hospital reputation, as we know it today in the U.S., is based on high-quality care and customer service.4,5
Since 1991, US News and World Report has published an annual list of America's Best Hospitals. They rank hospitals based on the Index of Hospital Quality (IHQ) and physician surveys.14 The methodology behind the IHQ was developed in the early 1990s by the National Research Opinion Center (NORC) at the University of Chicago. The IHQ reflects 14 factors, grouped under three interlocked dimensions of healthcare: structure, process, and outcomes. Their relationship in the methodology was described by Donabedian in a widely accepted model.18
Structure refers to resources directly related to patient care: intensity of nurse staffing, competency of clinical staff, availability of desirable technologies, patient services, and special status conferred by a recognized external body. Processes of delivering care include diagnosis, treatment, prevention, and patient education. Structure and process produce outcomes, the most obvious of which is whether a patient lives or dies. These outcomes are measured by a risk-adjusted mortality rate (adjusted for severity of diseases) and by related indicators such as complications, readmissions, patient safety, and infection rates. These could be collectively called "quality of medical care".5
According to Merrill, third-party generated hospital reputation scores impact patient volume, as patients obviously tend to choose hospitals with good reputations.4 She quotes Rao to demonstrate that reputational credentialing is another factor that affects hospital reputation.19 Rao points out that third parties such as professional societies, rating agencies, auditors, and governmental regulators may endorse an organization and that the very act of endorsement embeds an organization in a status hierarchy.19 That of course builds the reputation of the organization. Hospitals use reputation rankings to draw patients to their facilities. According to Merrill, a hospital's reputation provides a competitive advantage to draw patients to their centers, but on the other hand it provides patients an indicator of quality when selecting hospitals for their care.4 It is not uncommon for patients who have a terminal illness or complex disease to be willing to travel to a hospital known for its reputation, regardless of distance.6
For the purpose of this study, we concur with the widely accepted notion that the reputation of a hospital is a reflection of its quality. Dollinger et al.20 call it "product quality," which in the case of a hospital could be translated to the delivery of care and its outcome. Therefore, we define reputation as the quality of medical care based on its past performance.
Physicians tend to refer their patients to hospitals (physician referral) where they know the staff and where the hospital has a good reputation.21 Physicians also may choose a hospital based on its reputational score assigned by US News and World Report.4 Similarly, patients tend to choose a hospital known for its high-quality care.
This leads us to the first hypothesis.
Hypothesis 1: Reputation of a hospital will have a positive impact on a patient's choice of the hospital; higher the reputation better the chice.
2.2 Cost
Much work has been done to understand the relationship between purchase intention and value. Leszinski and Mann define value as the trade-off between customers' perceptions of benefits received and sacrifices (cost) incurred.22 Value consists of both cost
and benefits. In America, majority of the cost of medical care is borne by employers or through public programs such as Medicare and Medicaid. Therefore, for the purpose of this study, cost of care consists of out-of-pocket expenses such as cost of travel, food, and lodging and co-pays and deductibles, which can be grouped under the term "economic cost".
Cost of treatment may vary based on where you receive the treatment or the stage of the disease, or the insurance product you subscribe. For example, terminally ill patients might require a number of treatments to keep the disease from progressing and to keep them comfortable. Low-cost treatment options may be available more readily in developing countries compared to developed countries, which involves long-distance travel.
In a study conducted on the Thai hospital system, Srivoravilai et al. observed that the hospital's main target audience is comprised of Thai nationals and foreigners in search of affordable medical treatment.8 Currently, Thai nationals account for 60% of their customer base. Foreigners from 136 countries, mainly from the Middle East and southern and eastern African countries, account for 40%. Thus, it is clear that when it comes to choosing a hospital, patients do consider cost as an important factor in their decision- making process. For the purpose this study, we define cost as the economic sacrifice patients incur to receive medical care. The previous findings lead us to the second hypothesis.
Hypothesis 2: Cost of care has an impact on a patient's choice of a hospital; the higher the cost, the lesser will be the choice.
2.3 Distance
Early studies of hospital choice reported that distance to a hospital was an important factor.1 Wolinsky and Kurz reported on nearness to home, an important factor for patient choice of a hospital.2 According to Lee et al., the National Opinion Research Center (NORC) studied hospital selection factors in 1984, 1985, and 1986; "close to home" was one of the factors listed as having an impact on hospital choice.5
Although patients prefer to be treated closer to home, when faced with a terminal and incurable disease like cancer, some patients might be willing to travel to a hospital with a great reputation, regardless of distance and cost.6 A reason why cancer patients may hesitate to travel, however, is physical weakness. Rosenbaum et al. report that fatigue is the leading symptom reported by cancer patients undergoing medical treatment. 13As a result, some patients choose not to travel to destination hospitals but access treatment in hospitals closer to home. Many patients report emotional difficulty and physical symptoms associated with travel to a cancer center away from home.15
In addition to their physical, medical, and economic needs, cancer patients and their caregivers have social and emotional needs.5 Going away from home can compromise the opportunity to meet those needs. Although Payne et al. indicate that it is premature to conclude that travel distance and difficulty enhance psychological distress, they agree that many cancer patients find it inconvenient and adverse.23 Quoting Carlson and Hamrin, 24Payne et al. reported that social support is important for psychological adjustment and survival for breast cancer patients.23 For the purpose of this study, the authors define distance as long physical distance and the issues associated with it, such as fatigue as well as social and emotional needs.5 This leads us to the third hypothesis.
Hypothesis 3: Distance has a direct and negative impact on a patient's choice of a hospital; the longer the distance, the lesser will be the choice.
2.4 Servicescape
The concept of servicescape was developed by Booms and Bitner to identify the impact of a physical environment in which service processes take place.25 They refer to servicescape as the environment in which the service is assembled and in which the seller and customer interact, combined with tangible commodities that facilitate performance or communication of the service. 25 Bitner coined the term "servicescape" to define the built environment that affects both consumers and employees in service organizations.11 According to Bitner, servicescapes may elicit emotional responses that in turn influence behaviors.
As the service industry has grown tremendously in the past few decades12, much attention has been devoted to understanding how the physical environment influences experienced and inexperienced customers. Similarly, Kotler's work is based on atmospherics: the atmosphere of a particular set of surroundings is described in sensory terms.26 Kotler defines atmospherics as the effort to design buying environments to produce in the buyer specific emotional affects that enhance purchase ability. The sensory channels for atmosphere are light, sound, scent, and touch. Kotler argues that the atmosphere can affect purchase behavior as it may arouse visceral reactions that can contribute to purchase probability.
Scientific theories indicate that the inner world of human beings -their thoughts, feelings, and hopes - form their outer behavior.27 According to Mari and Poggesi, there are three emotional states: pleasure/displeasure, arousal/non-arousal, and dominance/submissiveness (PAD)12, and these mediate responses to the environment in approach or avoidance behavior. Inner satisfaction is the result of outer behavior's response to the inner stimuli of the organism (stimulus-organism-response). According to Nord and Peter external stimuli that elicit positive responses can be paired with a product itself, eliciting a positive effect.28 Consequently, behavior may be altered, bringing the potential customer closer to the product. For example, a tired and weak cancer patient watching a commercial about a cancer hospital in the Bahamas could pair the thought of tiredness with a relaxing environment and eventually choose that hospital for treatment.
Oldenburg pointed out that offering patients living with cancer, their family members, and caregiver opportunities of a "third-place" can promote restoration and well-being.29
Oldenburg describes a hierarchy of places with home as the first place, work as the second, and a gathering place for pleasure as the third place. Based on Oldenburg's work, Huelat et al postulated that we should create healing environments for patients and providers that act as the third place, a simple place with elements of comfort, accommodating space, where people feel comfortable and welcomed rather than intrusion into the care routine.30 Elements of comfort and hope can be created by selecting naturally blessed locations for the company/hospital, creating a physical space conducive to comfort, and a workforce gifted in customer care. The idea of such a place is incorporated in the work of Bitner, generally known as servicescape.11
According to Bitner, the servicescape includes the facility's manufactured or built exterior (landscape, exterior design, signage, parking, surrounding environment) and interior (interior design and decor, equipment, signage, and ambiance).11 Drawing from the work of Mehrabian and Russell, Bitner points out that any environment, natural or manmade, can be located in a two-dimensional space (pleasure-displeasure and degree of arousal)
reflecting peoples' emotional response to the place. 31Customers would want to spend time and money where the environment elicits feelings of pleasure.
Bitner's study concluded with the following observations. First, the servicescape provides a visual metaphor for an organization's total offering, suggesting the potential usage and relative quality of the service. Second, the servicescape can assume a facilitator role either aiding or hindering customers' ability to carry out their activities. As a facilitator, the servicescape can also encourage and nurture certain forms of social interaction among patients that can strengthen their approach behavior. In fact, Bitner suggests that major changes in physical design or the planning of new environments should be done with input from actual users (employees and customers), as it impacts customer attraction and satisfaction.11
For the purpose of this study, we define servicescape as the environment in which the service is assembled and in which the customer and employer interact to facilitate service delivery. The environment constitutes both the external and internal environments. By "external environment," we mean the manufactured exterior of the hospital. The internal environment consists of the manufactured interior space of the hospital, signage, and ambiance. A superior servicescape can be defined as one that has an appealing environment in which service is assembled and delivered by a highly competent and customer-oriented team. It also moderates the negative impact of issues associated with long-distance travel, which leads us to the next two hypotheses.
Hypothesis 4: Servicescape impacts a patient's choice of a hospital; the more superior the servicescape, the better the choice.
Hypothesis 5: A superior servicescape has a positive moderating effect on the negative relationship between distance and hospital choice; the more superior the servicescape, the less the negative impact of distance upon choice.
2.5 Patient Choice
Patient choice is the focal dependent variable for this study. Patient choice was selected as the focal outcome variable because it is, of course, necessary for hospital survival among a strong set of competitors. In order to understand the patient choice concept, we reviewed the study of Jung et al.,17 which used a hypothetical future choice model. They indicated that certain types of quality can be evaluated only by experience. For example, how well a nursing staff treats patients with respect can be evaluated only by having that experience.
Consumer choice of a hospital occurs in two stages - initial choice and subsequent choice. For most terminally ill patients (i.e., cancer patients), choice would include both stages since treatment occurs through multiple hospital encounters. For the purpose of this study, we will survey cancer patients who were treated as in-patients or out-patients at least one time. Respondents will be asked to make a hypothetical future choice such as "Would you use this hospital in case you need future hospitalization, or would you recommend this hospital to a friend or a relative?" We define hospital as both the in-patient facility and the out-patient clinic where respondents have received treatment in the past, and choice as the patient's desire to select a hospital for current or potential future care or recommending the hospital to someone else.32 The full model is presented in Figure 1.
Figure 1.

3. METHODOLOGY
3.1 Research Context
We chose to test the relationship of the conceptual model in a cancer hospital, specifically a destination cancer hospital. Our rationale for selecting a destination hospital for study evolves from the fact we intend to study not only the impact of servicescape in choosing a hospital, but also to test its moderating impact on long-distance travel concerns. A disease such as cancer can be treated only by certain hospitals or physicians. Therefore, reputation of the hospital is an important factor in the choice-making process. Although, in most instances, cost of care is covered by some type of health insurance, the cost of cancer treatment is very high. Even the co-pays and deductibles may be out of reach or burdensome for many patients.
The impact of physical space in a cancer hospital on its patients cannot be overemphasized as cancer patients spend a great deal of time in a hospital environment compared to patients with most other diseases. Patients' encounters with hospitals in many disease cases are one time or a limited number of times, as the disease can be cured or controlled by a few encounters. On the other hand, cancer patients' encounters with the hospital are multiple times over a period of months if not years. Practice management experts estimate cancer patients' consumption rate as seven to ten times higher than a regular patient's consumption of services. Because the service is produced and consumed simultaneously, the patient is "in the factory" experiencing the total service within the hospital's physical facility11 - all the more reason to have a third-place physical environment. Rosenbaum et al. studied the impact of restorative servicescapes on cancer patients with cancer-related fatigue and reported that cancer patients undergo restoration from those symptoms when at home-like cancer resource centers.13
The hospitality industry has successfully overcome the negative impact of long-distance travel and is in fact wildly successful in motivating people to travel long distance to access their facilities by making the physical space attractive and relaxing, locating them in attractive natural settings, and serving them with staff gifted with extraordinary service skills. We believe that a destination cancer hospital with its superior servicescape will have the same time type of impact on its customers, the cancer patients. Mari and Poggessi confirmed that it is possible to influence customer behavior through manipulating a store's servicescape.12 We believe that it is possible to influence a cancer patient's behavior of choice of hospital by manipulating the hospital's servicescape. For all of the above reasons, we argue that a cancer hospital provides an excellent context to test these constructs: reputation, cost, distance, and servicescape.
3.2 Design - Item Generation
To compile the scale on "reputation," we used three articles: Gardberg and Fombrun,33 Tokunaga et al., 32 and US News and World Report.14 US News and World Report used the Index of Hospital Quality (IHQ) to rank America's best hospitals.14 They measured quality in three subdimensions: structure, process, and outcomes.34 We selected five items out of these three subdomains for scale development: competency of nursing staff, competency of physicians, desirable technologies, outcomes (indicative of improvement in health status), and third-party endorsement.
For the construct "cost," the four-item scale was developed from a study conducted in 2013 by the consulting firm on a cancer specialty hospital. We selected four items for measurement: in-network insurance, transportation, food, and lodging costs.
Items for the construct "distance" were developed from Lightfoot et al.,15 Hooper and Coughlan16, and Rosenbaum and Smallwood 13. We added an item to the distance construct - travel from home to cancer center was physically challenging - to reflect the physical impact of long-distance travel. The parameters selected for measurement are physical, social, and economic challenges associated with long-distance travel.
Items for the construct "sevicescape" were developed from Lightfoot et al.,15 Hooper and Coughlan, 16 and Rosenbaum and Smallwood.13 To measure the manufactured physical environment of the servicescape, we selected parameters such as physical appearance of the plant (external and internal), signage, and ambiance.
For the dependent variable "patient choice," we used the hospital attributes from the studies of Jung et al. 17 and Tokunaga et al. regarding choice as a hypothetical choice related to current or future need and willingness to recommend the hospital to a friend or a relative.32
A total of 28 items were selected for the four independent variables, the dependent variable, and the control variable. These items were reviewed by a group of subject matter experts. A survey tool consisting of 40 questions was developed from these items, 30 questions for the four constructs, two questions for the dependent variable "patient choice," three questions for the control variable "patient satisfaction" and five demographic questions. Following Hinkin's directions35, we maintained four to six items per construct, while maintaining a simple structure, or parsimony. Respondents were asked to indicate the extent to which they agree with each item on a five-point Likert scale, (1) strongly disagree to (5) strongly agree.
3.3 Control Variable
Knowing that patient satisfaction has an impact on a patient's choice of a hospital,32 we selected patient satisfaction as the control variable. The impact of the four constructs - reputation, cost, distance, and servicescape- will be studied, controlling for patient satisfaction (given that we are predicting future choice of hospital). We will thus be able to ensure that the choice of the hospital is truly due to the impact of the constructs under
study, and not due to an overwhelming satisfaction with the place due to other factors such as religious affiliation or familiarity with senior administration and physicians.
3.4 Main Study
3.4.1 Sample
Data for the study was collected from patients diagnosed with some type of cancer, age 20 or older, both male and female, living in different parts of the country. While one set of subjects was selected from a central file of patients, another set of subjects was selected from one of the hospitals while they ere on-site for treatment. The patients selected did have at least one treatment encounter in an in-patient or out-patient cancer clinic. Since the selected hospitals are destination hospitals, patients from all over the country and even from other countries access these hospitals for treatment, providing the selected sample a good representation of diversity among patients.
3.4.2 Procedure
The survey was delivered to 687 patients; 483 were sent electronically through Survey Monkey and the remaining 204 were hand-delivered to active patients who were on-site in the hospital. The survey was administered and collected by personnel from the hospital's survey department. A cover letter was included with the survey informing the respondents that participation in the survey was completely voluntary and that the returned surveys had no tracers, thus maintaining confidentiality. Of the 687 surveys delivered, 332 were returned, resulting in a 48.3% response rate. However, only 305 were included in the analysis, as the remaining responses were rejected due to incompleteness. Data points were incorporated into Excel for future analysis and reviewed to ensure completeness. The 305 completed responses exceed the item-to-response ratio of 1:4 suggested by Rummel37 but falls below the 1:10 ratio suggested by Schwab38. However, recent research suggests that a sample size of 150 observations is enough to obtain an accurate solution in Exploratory Factor Analysis (EFA) and that 200 sample observations is enough for an accurate solution in confirmatory factor analysis (CFA).35 Therefore, a sample size of 305 is well justified for an accurate solution.
3.4.3 Survey Response Construct Measures Analysis
The construct measures analysis consisted of evaluating the measurements to ensure acceptable reliability of the measures, acceptable validity between measures, as well as the expected factor structure. Before evaluating the factor structure, we reviewed descriptive statistics for missing data, distribution, and demographics as they form the basis of virtually every quantitative analysis of data. The analysis shows that there is very little missing data for any question.
Once the data was collected and reviewed, factor analysis was used to further refine the measures, creating a more parsimonious representation of the original set of observations and providing evidence of construct validity.35 Both EFA and CFA were utilized to evaluate the factor structure. Both regression analysis and structural equation modeling were used to do hypotheses testing.
Prior to performing factor analysis, we evaluated the appropriateness of applying factor analysis by measuring sample adequacy (MSA) by using Kaiser-Myer-Olkin (KMO) and Bartlett's test of sphericity. Interpretive adjectives for the Kaiser-Meyer-Olkin (KMO)
Measure of Sampling Adequacy are: in the 0.90's as marvelous, in the 0.80's as meritorious, in the 0.70's as middling, in the 0.60's as mediocre, in the 0.50's as miserable, and below 0.50 as unacceptable
The value of the KMO Measure of Sampling Adequacy for this set of variables is .796, which if rounded off to two decimels would be equal to .80, labeled as "meritorious." Since the KMO Measure of Sampling Adequacy meets the minimum criteria, we did not examine the Anti-Image Correlation Matrix. Bartlett's Test of Sphericity tests the hypothesis that the correlation matrix is an identity matrix; all diagonal elements are 1 and all off-diagonal elements are 0, implying that all of the variables are uncorrelated. The Significance value for the analysisis is .000. Therefore, the null hypothesis is rejected, and the conclusion is made that there are correlations in the data set that are appropriate for factor analysis.
In addition, as suggested by Kim and Muller39, we performed factor analysis using Principal Axis Factor (PAF) to examine the inter-item correlation of the variables. As per Hinkin's recommendation35, variables loading greater than .40 were retained. All the variables in the study met this criterion except Variables 6, 19, and 22. Question 6 is an insurance question, and Q 22 is about hospital cleanliness. Neither question is relevant to these patients as insurance pays the bulk of their cost and the selected hospitals are very clean. Variable 19 is for directional signs, which is part of Bitner's original concept of servicescape.11
Four factors were extracted for variables associated with servicescape: factor 1 is an employee factor, factor 2 physical environment, factor 3 natural environment, and factor 4 social environment. Variables 19 and 22 had loadings less than .4. Variable 19 is for directional signs, which is part of Bitner's original concept of servicescape; as such we decided to retain it for analysis. We removed Variable 22 from the analysis; it is a cleanliness question that is irrelevant to the patients as the facilities are kept very clean.
PAF analysis indicated the presence of nine factors. All the variables loaded on appropriate factors except Variable 35 (patient satisfaction), which was loaded on factors 6 and 7. However, loading on factor 6 (.761) is acceptable since it is the appropriate factor and is twice as strong as factor 7(.361)35, establishing its higher correlation to factor 6. In summary, the selected variables represent the content domain of the underlying construct. The total variance explained is at 67.35%, which exceeds the 60% minimum acceptable suggested by Hinkin.35
According to Price and Meuller40, the most accepted measure for reliability is the internal consistency reliability measure Cronbach's alpha. Cortina41 recommends the use of this statistic in conjunction with factor analysis. A large coefficient alpha of .7 or higher is considered an indication of strong covariance and suggests that the sampling domain has been captured adequately. All the alphas here are .739 or higher, indicating high reliability. A summary of these values is provided in Table 2.

CFA was done using SPSS/AMOS software. Hinkin suggested the use of chi-square to measure the model fit.35 According to Hinkin, the smaller the chi-square the better the fit of the model.35 He points out that a chi-square two or three times as large as the degrees of freedom is acceptable as an indication of good model fit. However, as chi-square measure is sensitive to sample size, it has been suggested that the chi-square statistic be used with caution, and indicies such as Comparative Fit Index (CFI) be included.36 Based on their recommendation we used other indices, which, along with the CFA results, are summarized in Table 3. Although not all findings strongly support good fit, most of the observed findings indicate acceptable model fit.

4 FINDINGS
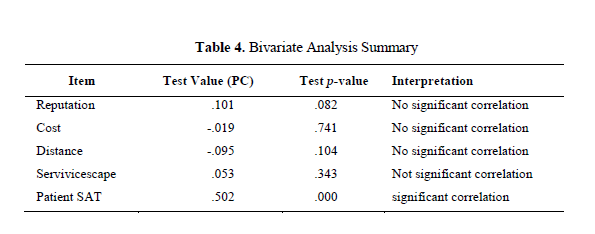
4.1 Bivariate Analysis Results
Data for the study was collected from 305 cancer patients. Bivariate analysis indicates that there is no correlation between the four independent variables (reputation, cost, distance, and servicescape) and the dependent variable patient choice. However, the results indicated good correlation between patient satisfaction and patient choice (r = .502, p < .001). The results are summarized in Table 4.
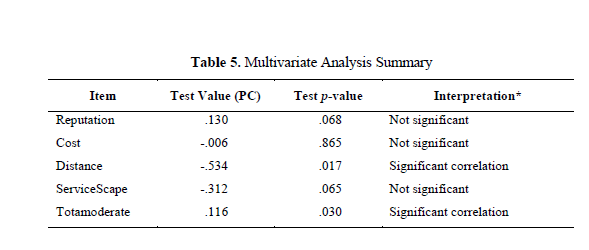
4.2 Multivariate Analysis Results - Patient Choice
In the multivariate analysis, four direct and one moderated relationship were tested using multiple regression analysis. The non-moderated relations include reputation and patient choice, cost and patient choice, distance and patient choice, and servicescape and patient choice. The moderated relations include servicescape total moderation and distance. Initially we ran the four factors and servicescape total moderation, including demographic variables, to predict patient choice, but patient satisfaction was not included. The overall model is significant as the p-value is .035. At the usual p-value < .05 level, only the distance factor is significant, which is negatively correlated with patient choice. Servicescape moderation is also significant and is positively correlated with patient choice. The results are summarized in Table 5.
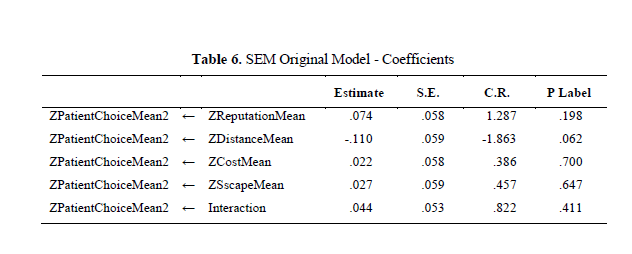
4.3 Structural Equation Modeling (SEM) Original Model - Hypothesis Testing
In order to better understand the interactions and examine the effects of the various constructs of patient choice, a structural equation model approach using SPSS was utilized. First, the original proposed patient choice model was analyzed using SEM without controlling for patient satisfaction. The four non-moderated relations were reputation and patient choice, cost and patient choice, distance and patient choice, and servicescape and patient choice. In addition, servicescape and distance moderation was also tested.
According to Hooper et al.,42 there are three types of test categories that measure goodness of fit; absolute fit, incremental fit, and parsimonious fit. They point out that although there are many indices to report and there is no golden rule to assess goodness of fit, it is necessary to report a variety of them. Based on the many published suggestions, Hooper et al.42 suggested that it is sensible to include the χ2 statistic, its degrees of freedom and its p-value, RMSEA and its associated confidence interval, the SRMR, the CFI, and one parsimony fit index such as the PNFI. These indices have been chosen over other indices as they have been found to be the most insensitive to sample size, model misspecification and parameter estimates.
The findings reported χ2 at 99.791 and DF 7, and the p-value < .001. According to Hooper et al,42 the chi-square statistic is sensitive to sample size. Therefore, researchers have sought alternatice indices to assess model fit. One such index that minimizes the impact of sample size on the Model Chi-square is relative/normed chi-square (χ2/df) Wheaton et al's 43. The recommended range for this statistic is 2-5.16 Since this study has a relatively small sample size, based on Wheaton et al's recommendation43, we used the relative/normed chi-square, instead of the Model Chi-square statistic to evaluate model fit, which is 14.26. The other SEM model fit indices, such as GFI = 899, AGFI = 698, comparative fit index (CFI) = 202, and root mean square error of approximation (RMSEA) = .212 are all less than the expected ranges, indicating poor model fit. The table of SEM coefficients (Table 6) demonstrates that none of the factors are significant at the usual p-value <0.05 level, indicating no significant correlation to patient choice.
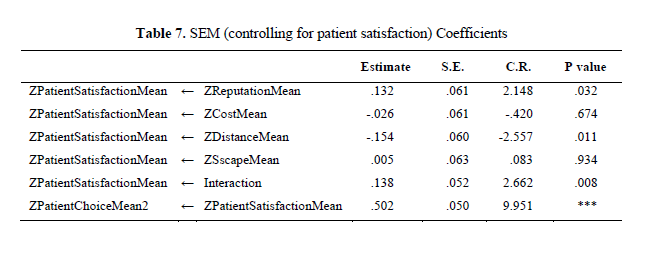
4.4 Structural Equation Modeling (SEM) Original Model - Controlling for Patient Satisfaction
As in the original model, four direct, non-moderated relationships and servicescape moderation on distance were tested using structural equation modeling. Since reputation, cost, distance, and servicescape did not have a direct impact on patient choice, based on the SEM results of the original model, the authors tested the model with reputation, cost, distance, servicescape, and servicescape moderation on distance as predicators of patient satisfaction and patient satisfaction as a predictor of patient choice.
The findings indicated χ2 = 21.320, degrees of freedom = 9, and probability level = .011. The realative/normed chi-square (χ2/df) is less than 2.4. The SEM fit indices GFI = .989, AGFI = .962, CFI = .982 and RMSEA = .040, indicating acceptable model fit. Results are shown in Table 7.
4.5 Individual Hypothesis Testing Results
H1 - Reputation: The first hypothesis was on reputation which stated that a hospital's reputation will have a positive impact on a patient choice of the hospital. The p-value is .032, which is significant, but in relation to patient satisfaction, which in turn is a predictor of patient choice.
H2 - Cost: Cost has a p-value of .674, which is not significant. The hypothesis is not supported.
H3 - Distance: Distance has a p-value of .011, which is significant, indicating distance has a negative impact on patient choice.
H4 -Servicescape: Servicescape has a p-value of .934, which is not significant. The hypothesis is not supported
H5 -Servicescape Moderation: The p-value for servicescape moderation is .008, which is significant. The hypothesis is supported that servicescape has a positive moderating effect on the negative impact of distance on patient choice.
5 DISCUSSIONS AND CONCLUSIONS
In this study, we looked to understand the impact of reputation, cost, distance, and servicescape on patient choice of a hospital. We also explored how a superior servicescape moderates the negative impact of distance on patient choice. A total of five hypotheses were developed to examine the impact of these factors. Bivariate, Multivariate, and SEM analysis were performed to validate them. We will discuss the implications of these results for both theory and practice, reflect on the limitations of the study, and provide possible areas of future research regarding servicescape applications.
5.1 Interpretation of Results
The three different kinds of analytical methods unfolded results in different ways. As the method complexity increased from bivariate to SEM, the clarity of the findings increased as well. Results from the bivariate analysis indicated that patient satisfaction had a significant correlation with patient choice and servicescape moderation had a significant correlation with distance. Other factors did not show significant correlation. Results from multiple regression analysis indicated that reputation had a borderline impact on patient satisfaction. Distance indicated a significant negative relationship with patient satisfaction, and servicescape moderation indicated a significant correlation with patient satisfaction as well. SEM results demonstrated additional relationships compared to what was demonstrated by bivariate and multiple regression analysis. First, we analyzed the data using the original proposed model. The results indicated that the original proposed model was not significant.
We repeated the analysis controlling for patient satisfaction, which resulted in acceptable model fit. These results confirmed that reputation had a positive and direct impact on patient satisfaction and consequently patient choice (partial support for H1). Cost did not have an impact on patient satisfaction (H2). Distance did have a significant and negative impact on patient satisfaction (H3). While servicescape did not have a significant impact upon patient satisfaction (H4) or patient choice, it certainly did have a significant moderating effect on the negative impact of travel on patient choice (H5).
As predicted, reputation had a significant and positive impact on patient satisfaction, which in turn had a significant impact on patient choice of a hospital. It was clearly evidenced in the literature review that in America high quality equates to reputation, and patients and
physicians alike choose hospitals with high reputation for treatment.<4,14>
Cost did not have a significant impact on patient satisfaction or choice. The result does not agree with the common notion that high cost has a negative impactor on patient choice. This does not necessarily mean that patients are not concerned about cost. A possible explanation is that most of the selected patients have insurance, which means less financial burden on the patients. Being a destination hospital, the hospital covered much of the out-of-pocket expenses such as food, transportation, and accommodation. Therefore, the high cost of care may not be a significant issue for patients of this hospital system.
Distance had a significant negative impact on patent satisfaction, indicating that patients like to be treated closer to home.2 The study clearly indicates that distance has a negative impact on patient satisfaction and consequently patient choice. Mitigating the negative impact of distance might help more patients travel to access care. This is a win-win situation for both patients and providers. For patients, this would enable them to access care that is not available to them in their local area. For destination hospitals, this would bring more patients to their hospitals.
The research question was, "is servicescape a driver of patient choice?" We will attempt to answer the question by examining the SEM results for servicescape (H4) and servicescape moderation (H5). Servicescape's impact was examined in two parts. First, its impact on patient choice, and second its impact act as a moderator to decrease the negative impact of travel on patient choice. Hypotheses 4 was designed to answer the first part. Hypothesis 5 was designed to answer the moderating effect of servicescape.
The results indicate that sevicescape did not have a direct impact on patient satisfaction or consequently patient choice. This finding is quite unexpected as one might naturally think that a superior servicescape would be attractive to patients. However, there are a few things to consider. Nearly 60-70% of the patients surveyed had complex or advanced (late stage) cancer. Two thirds of the patients surveyed were patients on active treatment. Depending upon their physical condition, the experience factor (servicescape) may not be as important as the cancer treatment itself.
However, it is quite evident that servicescape was considered very important in the context of long-distance travel (Figure 2). The results indicate that servicescape had a strong and positive moderating effect on the negative impact of distance on patient choice of a hospital (H5). Servicescape moderation is one of the cornerstone arguments of this study. As proved by the third hypothesis on distance, long distance has a negative impact on patient choice. Travelling long distance to access care is challenging to patients. A sick patient is already weak and travelling long distance can only make it worse. A manufactured, inviting physical setting is comforting, and soothing. So, a superior servicescape has a positive and direct moderating impact on the negative effect of long-distance travel on choice. The model also indicated strong positive relation between patient satisfaction and patient choice. The moderating effect is shown in Figure 2.
Figure 2.

5.2 Theoretical Implications
In conclusion, the research question, "is servicescape a driver of patient choice?" is well answered by the findings in Figure 2. It suggests that when servicescape is high, long distance has no effect on satisfaction. When servicescape is low, low distance creates significantly higher satisfaction than long distance. Therefore, a superior servicescape has a positive moderating effect on the negative impact of distance, and its highest impact is when people travel.
The study of servicescape is important from a theory development perspective. Among marketing academics, Bitner produced the seminal work on servicescape. Her study's focus was on the physical aspects of the servicescape and its impact in a retail setting. Since Bitner's original model of servicescape11, other variations of the model have evolved.12,13 However, retail settings were the most widely investigated.12 Therefore, Mari and Poggessi suggested extending the study to other service firms such as hotels, airports, hospitals.12 Our study is, therefore, an extension of investigating servicescape in a hospital setting. Also, there have not been a comprehensive study that combined both traditional factors of choice and servicescape domains. Therefore, this study addresses the gap in knowledge by integrating all these stimuli into one study contributing to the theory development of the servicescape domain outside the retail domain.
As mentioned earlier, since Bitner's original model of servicescape study was published, other variations of the model have evolved that include testing of social and natural stimuli.12,13 These stimuli, however, affect customer behavior within their consumption setting. Our study not only examines servicescape's impact within the consumption setting but also its interaction with domains outside the servicescape such as distance, further expanding the "expanded servicescape perspective" of Rosenbaum and Massiah.13
5.3 Managerial Implications
The primary focus of this study was to understand the impact of servicescape on patient choice, both directly and indirectly, by mitigating the negative impact of travel. It is quite clear that when it comes to long distance travel, patients consider servicescape to be of significant importance. But it is also quite clear that reputation has a significant impact on patient satisfaction - and that a good reputation is primarily the result of high quality. It is important for managers to understand that reputation and experience (servicescape) must go hand in hand for high patient satisfaction and consequently higher choice.
The study is important from the context of changing U.S. healthcare. The cost of healthcare in the U.S. has been skyrocketing in the past decade, forcing U.S. customers to consider international treatment options, mostly in the developing countries. It is interesting that these overseas hospitals not only provide affordable, high-quality care, they combine comfort/pleasure with care. These hospitals make every effort to provide treatment with a touch of class: hotel-like hospital buildings located in a resort setting, concierge services, state-of-the-art technology, and service delivered by a highly talented customer-oriented team, forcing U.S. hospitals to rethink the way they deliver care. Now that the study has confirmed that distance has a negative impact on patient satisfaction and that servicescape can moderate that effect, the study provides a framework for U.S. hospitals for the use of servicescape as a competitive advantage to attract more patients to their centers rather than losing them to foreign competitors.
5.4 Limitations of the Study and research opportunities
The study has several limitations. First, although the sample size was adequate for an accurate solution, it still is a small sample. Advancing the study with a larger sample size would strengthen the theoretical arguments behind this study.
Although the study was conducted selecting a sample from one nationwide hospital system. it still is a homogeneous sample. Including patients from other destination hospitals is a desirable next step.
Cancer is not the only type of destination hospital that involves travel. Patients travel long distance to hospitals specializing in knee, cardiac, and neuro surgeries. Including those samples in a study would enhance its generalizability. Patients are traveling more to international hospitals to receive care and including those samples would further enhance the generalizability of the study.
The study was conducted on patients who had at least one treatment in a hospital or clinic prior to treatment at the selected hospital system. The patient choice questions were based on a hypothetical future choice based on previous experience. This study did not include patients choosing a hospital for the first time, and therefore it is missing information on the impact of these drivers on first-time patients.
Majority of participants in this study were late-stage patients on active treatment. It would be interesting to use the same tool on a sample of early-stage patients to understand the impact of these drivers on their choice. Although cost did not have a significant impact on these participants, we believe cost is an important factor for healthcare researchers to consider. It would be interesting to repeat the study with samples of in-network insurance, out-of-
network insurance, and self-pay patients. It would also be interesting to test this study in countries where healthcare costs are funded by the government. Yet another opportunity to test the validity of these hypotheses exists in some of the Asian countries where it is the patients' responsibility to manage most of their own healthcare.
The study demonstrated that servicescape can moderate the negative impact of distance on customer satisfaction and choice. The study of servicescape opens up an array of research opportunities in many sectors of business and community in terms of servicescape interactions to modify existing behaviors. Building aircrafts with servicescape concepts (planescape) may promote international travel, or a unique "churchscape" may increase church attendance by drawing people from outside their locale. Factor analysis indicated the presence of four factors in the servicescape domain, resulting in additional opportunity to test their impact on patient choice.
This study moves the servicescape paradigm forward and supports an expanded conceptualization of the term. While so far researchers of servicescape have focused on studying the impact of servicescape stimuli on the behavior of customers within its consumption setting, this study's major focus was its interaction with factors external to it. The idea of a servicescape is to create a "Third Place" within a place or transform the whole place to a Third Place, a place where people look forward to gathering outside the familiar confines of the first and second places, home and workplace. Businesses that have embraced the value of becoming a known "Third Place" have adopted the concepts of servicescape and have prospered as a result.
REFERENCES
1. Porell, F.W., and E.K. Adams. "Hospital Choice Model:Review and Assessment of Their Utility for Policy Impact Analysis,"Medical Care and Research Review. 1995, 52(2), 158-195.
2. Wolinsky F.D., and R.S. Kurz. "How the Public Chooses and Views Hospitals," Hospital Health Services Administration. 1984, 29(6), 58-67.
3. Fottler, M., R. Ford, V. Roberts, and E. Ford "Creating a Healing Environment: The Importance of the Service Setting in the New Comsumer-Oriented Healthcare System," Journal of Healthcare Management. 2000, 45(2), 91-106.
4. Merrill, Sonya Butler. "Investigation of a Measure of Hospital Reputation," The Journal of Business, 2002, 75, 203-210.
5. Lee, Wan, Bih-Yaw Shih, Yi-Shun Chung. "The Exploration of Consumers' Behavior in Choosing Hospitals -By the Application of Neural Networks," Expert Systems with Applications. 2008, 34, 806-816.
6. Connel, John. "Contemporary Medical Tourism: Conceptualization, Culture and Co-Modification, Tourism Management, 2013. 34, 1-254.
7. Edelheit, J. Overseas Options. Managed Healthcare Executive. 2008.
8. Srivoravilai, N., T.C. Melewar, M. J. Liu, and N. Yannopoulou. "Value Marketing Through Corporate Reputation: An Empirical Investigation of Thai Hospitals," Journal of Marketing Management. 2011, 27(3-4), 243-268.
9. Jagyasi P. "Defining Medical Tourism - Another Approach," Medical Tourism Magazine.www.medicaltourismmag.com/issue-detail.php? item=136&issue=6. 2008.
10. Lee, Seunghae. "Evaluating Serviceability of Healthcare Servicescapes: Service Design Perspective," International Journal of Design. 2011, 5(2).
11. Bitner, Mary Jo. "Servicescapes: The Impact of Physical Surroundings on Customers and Employees," Journal of Marketing. 1992, 56, 57-61.
12. Mari, Michela, and Sara Poggesi. "Servicescape Cues and Customer Behavior: A SystameticLiterature Review and Research Agenda," The Service Imdustries Journal. 2013, 33(2), 171-199.
13. Rosenbaum, Mark.S., and Carolyn Massiah. "An Expanded Servicescape Perspective," Journal of Service Management. 2011, 22(4).
14. US News and World Report, health.usnews.com/health-news/.../2013/.../31. 2013
15. Lightfoot, N., S. Steggles, D. Gauthier-Frohlick, R. Arbour-Gagnon, M. Conlon, C. Inne, L. O'Bonsawin, and H. Merali. "Psychological, Physical, Social, and Economic Impact of Travelling Great Distances for Cancer Treatment," Current Oncology. 2005, 12(4), 1-7.
16. Hooper, Daire, and Coughlan, Joseph. The Serviscescape as an Antecedent to Service Quality and Behavioral Intentions," Journal of Services Marketing. 2013, 27(4), 271-280.
17. Jung, Kyoungrae, Roger Feldman, and Dennis Scanlon. "Where Would You Go for Your Next Hospitalization?" Journal of Health Economics. 2011, 30, 832-841.
18. Donabedian, A. "Evaluating the Quality of Medical Care," The Milbank Memorial Fund Quarterly, (1966), 44(3).
19. Rao, H. "The Social Construction of Reputation: Certification Contests, Legitimation, and the Survival of Organizations in the American Automobile Industry: 1895-1912," Strategic Management Journal. 1994, 15(S1), 29-44.DOI:10.1002/smj.4250150904.
20. Dollinger, Marc J., Peggy A.Golden, and ToddSaxton. (1997) "The Effect of Reputation on the Decision to Joint Venture," Strategic Management Journal. 18(2), 127-140. DOI: 10.102/(SICI) 097-0266(199702)18.
21. Moosbrugger, M. Unclogging the Physician Referral Network," Healthcare Executive.1988.
22. Leszinski, R., and M.V. Mann. "Setting Value, Not Price," The McKinsey Quarterly. 1997, 1, 99-115.
23. Payne, S., N. Jarrett, D. Jeffs, L. Brown. "Implications of Social Isolation During Cancer Treatment.The Implications of Residemce Away From Home During Cancer Treatment on Patients' Experience: A Comparative Study." Health & Place, 2001, 7, 273-282.
24. Carlsson, M., and E. Hamrin. "Psychological and Psychosocial Aspects of Breast Cancer Treatment," Cancer Nursing, 17(5), (1994), 418-428.
25. Booms, Bernard H. and Mary J. Bitner "Marketing Services by Managing Environment," Cornell Hotel and Restaurant Administration Quarterly, 23 May 1982, 35-49.
26. Kotler, P. "Atmospherics as a Marketing Tool," Journal of Marketing. 1973, 49 (4), 48-64.
27. Järvilehto, Timo. Integrative Physiological and Behavioral Science, ISSN 1053-881X, 10/1998, Volume 33, Issue 4, 1998, pp. 321 - 334
28. Nord, Walter R, J. Paul Peter. "A Behavior Modification Perspective on Marketing," Journal of Marketing. 1980, 44(2), 36.
29. Oldenburg, Ray. The Great Good Place, Boston: Da Capo Press. 1999.
30. Huelat, Barbara,Pochron,S & Raimondeau, P. Healing Environments, What's the proof? Medezyn, 2007.
31. Mehrabian, Albert, and James Russell. An Approach to Environmental Psychology, Cambridge, MA: Massachusetts Institute of Technology. 1974.
32. Tokunaga, J, Y.Imanaka, K. Nobutomo. "Effects of Patient Demands on Satisfaction with Japanese Hospital Care," International Journal for Quality in Health Care. 2000, 12(5), 395-401.
33. Gardberg, N.A. and C.J. Fombrun. "For Better or Worse - The Most Visible American Corporate Reputations," Corporate Reputation Review, 2002, 4(4), 303-307.
34. Olmsted, M.G., Emily Geisen, Joe Murphy, Denise Bell, Melissa Morley, Marshica Stanley "Methodology: Best Hospitals, 2014-15," U.S. News & World Report. 2014, July 14.
35. Hinkin, T.R. "A Brief Tutorial on the Development of Measures for Use in Survey Questionnaires," Organizational Research Methods. 1998, 1, 104.
36. Medsker, G. J., Williams, L.J., &Holohan, P. J. A review for current practices for evaluating causal models in organizational behavior and human resources management research, Journal of Management. (1994). 20, 439-464.
37. Rummel, R.J. Applied Factor Analysis. Evenston, IL: Northwesten University Press. 1970.
38. Schwab, D.P. "Construct Validity in Organizational Behavior." In B.M. Staw and L.L. Cummings (eds), Research in Organizational Behavior (Vol. 2). Greenwich CT: JAI Press.1980.
39. Kim, J.O., and C.W. Mueller Factor Analysis: Statistical Methods and Practical Issues. Thousand Oaks, CA: Sage. 1978.
40. Price, J.L., and C.W. Mueller. Handbook of Organizational Measurement. Marshfield MA: Pitman Publishing. 1986.
41. Cortina, Jose M. "What is Coefficient Alpha? An Examination of Theory and Applications," Journal of Applied Psychology (1993), 78(1), 98-104. DOI: 10.1037/0021-9010.78.1.98
42. Hooper, D., J. Coughlan, M. Mullen, M. "Structural Equation Modelling: Guidelines for Determining Model Fit," Electronic Journal ofBusiness Research Methods, 2008, 6(1), 53-60.
43. Wheaton, B., Muthen, B., Alwin, D., F., and Summers, G. "Assessing Reliability and Stability in Panel Models," Sociological Methodology. 1977, 8 (1), 84-136.
44. Rosenbaum, Mark S., and JillianA. Smallwood "Cancer Resource Centers: Transformational Services and Restorative Servicescapes," Journal of Marketing Management. 2011, 27(13-14), 1404-1425.
45. Rosenbaum, Mark S., Jillian A. Smallwood, and Jillian Sweeney. Restorative Cancer Resource Center Servicescapes," Managing Service Quality. 2011, 21(6), 599-616.