Cardiac Spiderman: A case of suspected myocarditis after Loxosceles envenomation
Jane Rubenstein, D.O., Oklahoma State University, Department of Internal Medicine, Tulsa OK
Luke Roberts, D.O., Oklahoma State University, Department of Internal Medicine, Tulsa OK
Taryn Haney, D.O., Oklahoma State University, Department of Internal Medicine, Tulsa OK
Dev Jaiswal D.O., Oklahoma State University, Department of Cardiovascular Medicine, Tulsa OK
Address for correspondence: Jane Rubenstein, DO
OSU Medical Center 744 W 9th St, Tulsa, OK, 74127
Email: jane.rubenstein@okstate.edu
The authors have no funding sources supporting this work.
The authors have no conflicts of interest to disclose.
Abstract:
Envenomation via spider bites from specific genera have been linked with a variety of tissue injury. Though rare, spider bites from the black widow or brown recluse spider have been associated with myocardial injury secondary to direct cardiotoxic effects. This effect can result in myocarditis. In this report, we discuss a case of suspected myocarditis due to a brown recluse spider bite with the presentation of chest pain and elevated cardiac biomarkers.
Key words: Loxosceles reclusa, myocarditis, arachnidism
Introduction:
Myocardial injury has been related to ischemia, toxins, anaphylaxis, and drugs. Arachnidism—a medical condition defined as envenomation by a spider bite and most often associated with the black widow spider—has also been implicated in myocardial injury. Myocarditis secondary to black widow spider bites have been described in previous literature. However, less frequently discussed are cases of myocarditis secondary to bites from the brown recluse spider, otherwise known as Loxosceles reclusa. 1,2
The main chemical in the Loxosceles venom is sphingomyelinase-D. Sphingomyelinase-D may lead to tissue necrosis which risks the development of hemolysis, disseminated intravascular coagulation, rhabdomyolysis, and acute renal failure after envenomation by Loxosceles reclusa.3,4 Necrosis may also occur within the myocardial cells with a direct cardiotoxic effect on cardiac myocytes.5 This case report represents an example of myocardial injury suspected to be due to a Loxosceles reclusa bite.
Case report:
A 60-year-old male, with only known past medical history of essential hypertension and non-oxygen-dependent chronic obstructive pulmonary disease, was transferred from an outlying facility’s emergency department with a chief complaint of chest pain that was worsening over four days leading up to his presentation. He described the pain as squeezing and tightness in nature. Additional symptoms included generalized fatigue, malaise, nausea, vomiting, diaphoresis, night sweats, weight loss of up to 10 pounds. During questioning, the patient did report a bite by a brown recluse spider proximal to his fourth digit of his right hand just prior to onset of his symptomatology. He described erythema and edema of the right hand along with purulent drainage from an opening. At the time of his presentation, the patient exhibited an abscess to this area measuring 0.59 x 0.52 x 0.22 cm on ultrasound. [Figure 1] The lesion appeared to be healing and without open lesion on examination.
Figure 1 Right hand abscess measuring approximately 0.59 x 0.52 x 0.22cm

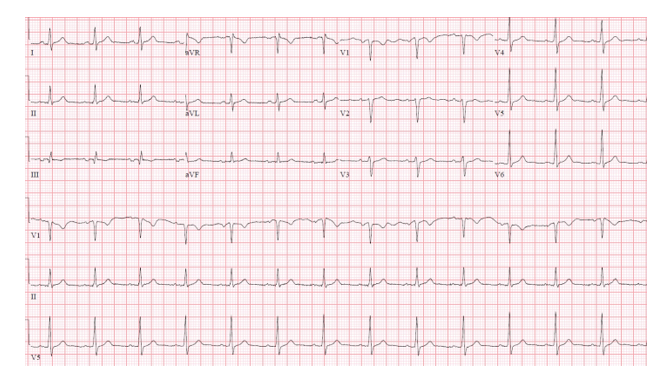
On initial evaluation at the outlying facility, the troponin was found to be greater than 3 ng/ml (reference range 0.00-0.04 ng/ml). At that time, his electrocardiogram revealed normal sinus rhythm with no acute ischemic changes. [Figure 2] Given his elevation in troponin and chest pain, the patient was transferred to our facility for cardiovascular services and any necessary management. On arrival, vital signs showed blood pressure 112/66, heart rate 85, temperature 36.8 ° Celsius, respirations 16. On examination he demonstrated a lesion on his right hand as described above. Laboratory analysis on admission showed white blood cell count of 12.5, hemoglobin 15.4, platelet count 304, creatinine 0.92, BUN 16, potassium 4, chloride 100, sodium 136, AST 51. A repeat troponin was also obtained. Results were 9.92 ng/ml, and a consultation was placed to the cardiology service. As the patient’s troponin continued to rise in the setting of persistent chest pain, a continuous heparin infusion was started, and the decision was made to perform urgent left heart catheterization.
Figure 2 Electrocardiogram showing normal sinus rhythm with nonspecific ST changes.
Left heart catheterization, it was revealed that the patient had moderate nonobstructive coronary artery disease involving the left anterior descending artery. Echocardiogram revealed an ejection fraction of 62%, normal left ventricular diastolic function, and a left ventricular end diastolic pressure of 23 mmHg. The troponin level was trended with a peak of 12.39 ng/ml. Erythrocyte sedimentation rate was found to be 82 mm/h and C-reactive protein 2.02 mg/dl leading to concern for myocarditis. The patient was started on clopidogrel, aspirin, atorvastatin, and carvedilol.
Additional evaluation during this patient’s hospitalization included consultation with orthopedic surgery for his abscess. It was determined that the patient would not need an incision and drainage and could be managed conservatively and therefore his wound was not cultured as it was no longer draining fluid. Blood cultures resulted without growth and the patient was continued on doxycycline monotherapy.
Unfortunately, the patient decided to leave the facility against medical advice while other apparent predisposing factors were being investigated for differential diagnosis of myocarditis versus vasospasm which further testing with cardiac magnetic resonance imaging.
Discussion:
Myocarditis can have varying presentations including fatigue, chest pain, heart failure, and arrhythmias. In this case report, the patient demonstrated a unique presentation of suspected myocarditis potentially caused by a Loxosceles reclusa bite. Additional etiologies for elevated troponin with the patient’s clinical presentation were considered including type one myocardial infarction and vasospastic event in the setting of substance use. A left heart catheterization performed upon admission revealed non-obstructive coronary artery disease. Additionally, though he did have a history of substance use, there was no clinical evidence to suggest active intoxication on presentation to our facility effectively making an acute vasospastic event less likely. Unfortunately, given his quick departure from our facility we were not provided the luxury of time to definitively diagnose myocarditis by way of cardiac magnetic resonance imaging or endomyocardial biopsy and his presentation was deemed to be most consistent with acute coronary syndrome-like acute myocarditis.6
In one study, it has been seen that mice injected with sphingomyelinase-D, which is present in Loxosceles reclusa venom developed myocardial injury represented by elevated creatine kinase-myocardial band levels.7 In this case, it is theorized the sphingomyelinase-D may have led to this cardiotoxic presentation. Other etiologies of elevated troponin in this patient could have been vasospastic in nature. Myocarditis was felt to be a more likely etiology in that the patient experienced a typical clinical presentation including acute chest pain, new onset fatigue and elevated troponin, exposure to toxic agent. Unfortunately, the patient left the facility prior to cardiovascular magnetic resonance which would have allowed for definitive diagnosis.
This patient’s skin lesion appeared consistent with descriptions of Loxosceles bite, he endorsed observation of the spider but was unable to recover it for further confirmation of genera. His wound originally presented as a papule with central pallor that later developed a dark center which is commonly seen.
Acknowledgments: The authors have no acknowledgments to disclose.
References:
1. Sims RA, Fish-Trotter HL, Clark DE, Gayle KA, Hughes SG, Brittain EL. Toxin-Mediated Myocarditis From Brown Recluse Spider Bite. JACC: Case Reports. Published online October 2021. doi:https://doi.org/10.1016/j.jaccas.2021.10.003
2. Piscopo A, Massari F, Scicchitano P, et al. Acute Myocarditis After Black Widow Spider Bite: A Case Report. Cardiology and Therapy. 2020;9(2):569-575. doi:https://doi.org/10.1007/s40119-020-00178-3
3. Robinson JR, Kennedy VE, Doss Y, Bastarache L, Denny J, Warner JL. Defining the complex phenotype of severe systemic loxoscelism using a large electronic health record cohort. Gutiérrez JM, ed. PLOS ONE. 2017;12(4):e0174941. doi: https://doi.org/10.1371/journal.pone.0174941
4. da Silva PH, da Silveira RB, Helena Appel M, Mangili OC, Gremski W, Veiga SS. Brown spiders and loxoscelism. Toxicon. 2004;44(7):693-709. doi:https://doi.org/10.1016/j.toxicon.2004.07.012
5. Anoka IA, Robb EL, Baker MB. Brown Recluse Spider Toxicity. PubMed. Published 2021. https://www.ncbi.nlm.nih.gov/books/NBK537045/
6. Ammirati E, Cipriani M, Moro C, et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients With Acute Myocarditis. Circulation. 2018;138(11):1088-1099. doi:https://doi.org/10.1161/circulationaha.118.035319
7. Dias-Lopes C, Felicori L, Guimarães G, et al. Cardiotoxic effects of Loxosceles intermedia spider venom and the recombinant venom toxin rLiD1. Toxicon. 2010;56(8):1426-1435. doi:https://doi.org/10.1016/j.toxicon.2010.08.008