Micah Hartwell, Ph.D., Office of Medical Student Research, Oklahoma State University College of Osteopathic Medicine at the Cherokee Nation, Tahlequah, Oklahoma Department of Psychiatry and Behavioral Sciences, Oklahoma State University Center for Health Sciences, Tulsa, Oklahoma
Jason Beaman, D.O., Department of Forensic Sciences, Oklahoma State University Center for Health Sciences, Tulsa, Oklahoma
Ashley Keener, Ph.D., Department of Health Care Administration, Oklahoma State University Center for Health Sciences, Tulsa, Oklahoma
Benjamin Greiner, D.O., M.P.H., Department of Internal Medicine, University of Texas Medical Branch, Galveston, Texas
Corresponding author: Swapnil Gajjar, Oklahoma State University Center for Health Sciences, 1111 W 17th St., Tulsa, OK 74107, United States. Email: sgajjar@okstate.edu, Phone: (918) 561-1844.
IRB Approval: Data used in this study was publicly available and contained no personally identifiable health information and was, therefore, precluded from IRB approval.
Abstract:
Background
Methamphetamine use can alter judgment and decision-making processes leading to sexually risky behaviors, such as unplanned unprotected sex, that may lead to sexually transmitted infections (STIs) including HIV. Thus, the objective of this study is to identify associations between HIV/STI testing and sexual violence among adolescents in the U.S. with and without a history of methamphetamine use.
Methods
We performed a cross-sectional analysis of the Youth Risk Behavior Survey System (2015-2019) to investigate associations between HIV/STI testing and sexual violence methamphetamine use among U.S. adolescents. We estimated prevalence of use by sociodemographic factors and calculated odds ratios, via logistic regression, to measure the associations between the variables of interest.
Results
Adolescents with methamphetamine use were more likely to complete HIV/STI testing compared to those who didn’t. Furthermore, in those who reported methamphetamine use, females were six times more likely, and males were ten times more likely to experience sexual violence compared to their counterparts without a history of methamphetamine use. Our study also found that the prevalence of methamphetamine use was higher among all groups of adolescents of Native American ancestry.
Conclusion
HIV/STI testing was significantly higher in adolescents who used methamphetamine than those who didn’t use it and were more likely to experience sexual violence; however, further research is needed to investigate potential interventions to reduce methamphetamine usage in U.S. high school students.
Key Words:
Methamphetamine, HIV/STI testing, adolescents, sexual violence, sexual-risk behaviors, drug abuse
1.0 Introduction:
According to Zapata et al,1 between 5-10% of high school students self-report lifetime MA use. The frequent use of MA often leads to a decline in psychological, social, and physical health, with the severity of this decline increasing in proportion to the dosage taken.2 Adolescence is a critical period for evaluating MA use due to its impact on lifelong behaviors.3 Adolescent brains are particularly vulnerable to MA, regardless of dosage or duration,4 potentially exacerbating impulsivity and risk-taking which may lead to such behaviors as unprotected sex, early sexual initiation, and inconsistent use of condoms and other barrier contraception.5,6 Consequently, these behaviors increase the risk for contracting Human Immunodeficiency Virus (HIV) among other Sexually Transmitted Infections (STIs)7—with HIV rates being six times higher among individuals who reported MA use alone compared to other substances.8 In 2016, approximately 30% of U.S high school students reported being sexually active, and among those youth, 43% had not used a condom during the last time they engaged in sexual intercourse.9 In light of both HIV and STI rates and the prevalence of sexual risk behaviors reported among youth, several clinical guidelines recommend testing youth for HIV and other STIs.10 Despite these recommendations, adolescents and young adults have relatively low rates for testing.10
A study published in 2008 assessed the association between MA use and sexual behavior among adolescents using data from 1993-2003 Youth Risk and Behavior Surveillance System (YRBSS);1however, we found no studies that have documented the association of MA use and sexual violence using the YRBSS since that time. Thus, the purpose of this study was to update the literature regarding sexual violence and MA use among adolescents in the U.S. and expand what is known about the relationship between MA use and HIV/STI testing among this group using data extracted from the Youth Risk and Behavior Surveillance System.
2.0 Materials and Methods
2.1 Data source
We performed a cross-sectional analysis of sexual violence and HIV/STI testing among U.S. adolescents reporting having used MA and those who haven’t using data extracted from the 2019 Youth Risk Behavior Surveillance Survey (YRBSS) National, State, and District Combined Datasets from 2015 to 2019.11 The YRBSS includes national, state, territorial and freely associated state, tribal government, and local school-based surveys that monitor priority health risk behaviors of representative samples of 9th through 12th-grade students in public and private schools in the US.11 These surveys are conducted every two years, usually during the spring semester. In addition, the YRBSS monitors health-related behaviors plus sexual identity and sex of sexual contacts.11 The methodology used in this study was submitted for ethics review via an institutional review board, but was determined to be non-human subjects research.
2.2 Questions items
Respondents were classified as having used MA if they responded “1 or more times” to the following: “During your life, how many times have you used methamphetamines (also called speed, crystal meth, crank, ice, or meth)?”. Respondents were categorized as never had used MA if they responded “0 times” to the above question. Respondents were classified as having been tested for HIV/STD if they responded “Yes” to either of the following questions: “Have you ever been tested for HIV, the virus that causes AIDS?” or “During the past 12 months, have you been tested for a sexually transmitted disease (STD) other than HIV, such as chlamydia or gonorrhea?” Respondents were classified as having experienced sexual violence if they responded “Yes” to the following question: “Have you ever been physically forced to have sexual intercourse when you did not want to?” or if they responded “1 or more times” for the following questions: “During the past 12 months, how many times did anyone force you to do sexual things that you did not want to do?” or “During the past 12 months, how many times did someone you were dating or going out with force you to do sexual things that you did not want to do?”. Respondents were categorized as never having experienced sexual violence if they responded “No” or “0 times” to the above questions. Pre-coded race categories were used in this study: American Indian/Alaska Native, Asian, Black or African American, Hispanic/Latino, Native Hawaiian/Other Pacific Islander, White, Multiple Races (Non-Hispanic). Data extracted also included sociodemographic variables. Missing data were excluded from the analysis.
2.3 Statistical analysis
Statistical analyses were performed on HIV/STI testing and sexual violence using Stata 16.1 software. Sample weighting was provided by the YRBSS. We then calculated prevalence estimates and corresponding 95% confidence intervals to describe sociodemographic variables among adolescents who used MA and those who have not. Multivariate logistic regression models were then constructed to assess the adjusted odds ratio for HIV/STI testing, and experience sexual violence. The regression models were controlled for age, gender, and race. We checked for interactions between MA use and gender and reported as needed.
3.0 Results
3.1 Sociodemographic Variables
Among the included participants (n = 40,722), the prevalence of MA use was 2.57% (n=1,235; Table 1). By ethnoracial groups, MA use was highest among respondents reporting as Hispanic (n=427) followed by White (n=374) and Black/African American. Among participants with MA use, approximately 65% were between the age of 15-17 (Table 1), with a majority being male (61%; n=757).
3.2 HIV/STI Testing & Sexual violence
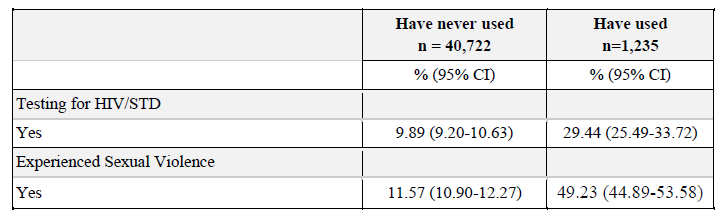
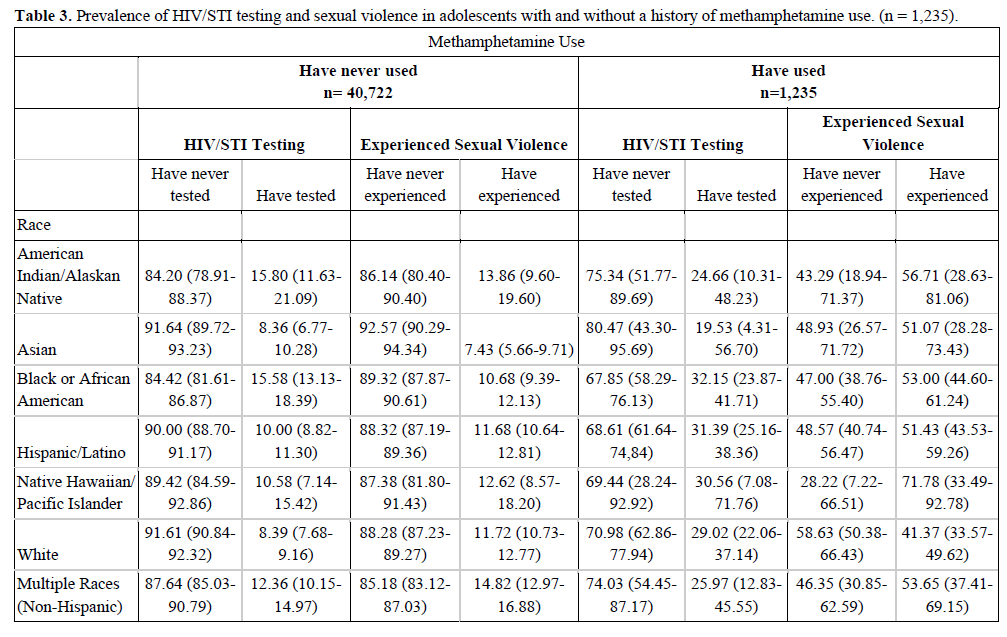
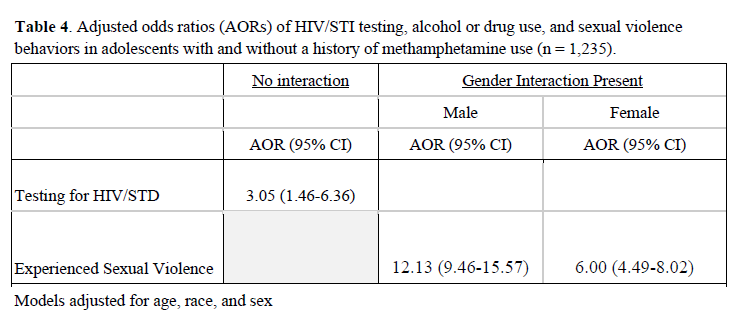
Our results showed the likelihood that participants who tested for HIV/STIs given MA use was significantly higher than those reporting no MA use (AOR 3.05; 95%CI: 1.46 - 6.36; Tables 2 and 3). Prevalence of testing for HIV/STIs was higher among participants with MA use (29.44%; 95%CI: 25.49 - 33.72) as compared to those without MA use (9.89%; 95%CI: 9.20 - 10.63). Among respondents reporting MA use, the prevalence of sexual violence was higher (49.23%; 95%CI: 44.89 - 53.58) than in those without MA use (11.57%; 95%CI: 10.90 - 12.27). When considering MA use in relation to ethnicity, the occurrence of sexual violence was more prevalent among individuals of American Indian/Alaskan Native and Pacific Islander/Hawaiian Native descent (71.78%; 95%CI: 33.49 - 92.7). The prevalence of sexual violence among males given MA use was higher than those without MA use (42.78%; 95%CI: 37.72 - 48.00). The prevalence of sexual violence among females given MA use was higher than those without MA use (58.52%; 95%CI: 51.63 - 65.09). Due to the interaction between gender and MA use, the likelihood of MA use for males was 12.13 (95%CI: 9.46 - 15.57) and the likelihood for females was 6.00 (95%CI: 4.49 - 8.02) among respondents who experienced sexual violence (Table 4).
4.0 Discussion
Our findings showed that respondents using MA were more likely to complete HIV/STI testing and are at more risk of experiencing sexual violence than those with no MA use. Overall, females were more likely to experience sexual violence with and without MA use; however, males who used MA were 12 times more likely to experience sexual violence than those who didn’t use MA and females were 6 times more likely to experience sexual violence than those with no MA use. This is the first study to date that identified associations between HIV/STI testing and sexual violence among adolescents with MA use among a nationally representative sample.
Youth MA use is a critical national public health problem, with 7.6% of US high school students1 reporting ever using MA, translating to more than 1 million adolescents nationwide. Almost half of the youth ages 18-24 living with HIV in the U.S. do not know that they are infected.12 Yet, our results indicate that HIV testing rates are low and other research shows13 they are not increasing among the adolescent population regardless of sexual behavior, race/ethnicity, and gender. Our study also identified that the prevalence of HIV/STI testing in adolescents with MA use is significantly higher than those who don’t use MA. Aligned with our results, another study found that people who use MA may be at higher risky for engagement in various sexual risk behaviors.5 The positive association between MA use and sexual risk behaviors may be due to the belief that MA enhances the sexual experience, as suggested in studies that have explored reasons and personal motivations for MA use with men who have sex with men (MSM)14,15 and heterosexual adults.16 The transmission of HIV/STIs has been associated with alcohol or drug use before sexual intercourse.17
According to a study by Yen,18 people with a history of MA use are more likely to engage in unplanned sex under the influence of alcohol as compared to those without MA use. A similar study also documents that the likelihood for adolescents engaging in most sexual risk behaviors examined tended to increase with a higher frequency of MA use.5 The relationship between MA use among adolescents and sexual risk behaviors may be a result of perceived enhancement in sexual experiences while intoxicated.19
While MA use has a reputation for inducing aggressive and violent behaviors, many individuals who use MAs appear to have developmental histories of physical and sexual abuse.20 A study published by Leslie et al21 documented a significant association between MA-related aggression and recurrent risky simultaneous methamphetamine and alcohol use. Our findings suggest a strong association between adolescents with a history of MA use and the likelihood of experiencing sexual violence as compared to those with no MA use. Further, we found out that male and female adolescents who used MA were more likely to experience sexual violence than those with no MA use which has been reported in other research. The sexual characteristics associated with MA use may result in more frequent sexual experimentation which may lead to increased risk of HIV/STIs and unwanted teenage pregnancy.20 Thus, effective, culturally appropriate education for adolescents about MA and treating MA-dependent adolescents may be an alternative to reduce the spread of HIV/STIs.
Limitations
Limitations to our study included the possibility of response bias as the data was self-reported. The YRBSS overall response rate between 2015-2019 was roughly 60% which is sufficient but may affect overall generalization. Within the data, we found that respondents under the age of 12 reported unusually high rates of methamphetamine use; however, the total number of individuals in this category is extremely small—accounting for only 0.26% of the sample and has a very limited impact on our findings. Further, as this is a cross-sectional analysis, causal inferences cannot be determined— only correlations. Strengths of using YRBSS include the large sample size and robust sampling techniques making this an appropriate dataset for our study.
5.0 Conclusion
Our findings suggest that adolescents with MA use were more likely to test for HIV/STIs as compared to those who don’t use MA. Moreover, American Indian/Alaskan Native and Native Hawaiian/Pacific Islander adolescents were at a higher risk for MA use and were more likely to experience sexual violence. We identified a significant association between MA use and violent and sexually risky behaviors; a factor that likely contributes to higher rates of HIV/STIs among adolescents who use MA. Although participants who used MA had higher rates of HIV/STI testing, our study suggests greater efforts are warranted to prevent and reduce amphetamine usage in adolescents.
6.0 Tables
Table 1. Sociodemographic factors in adolescents with and without a history of methamphetamine use (n=1,235)
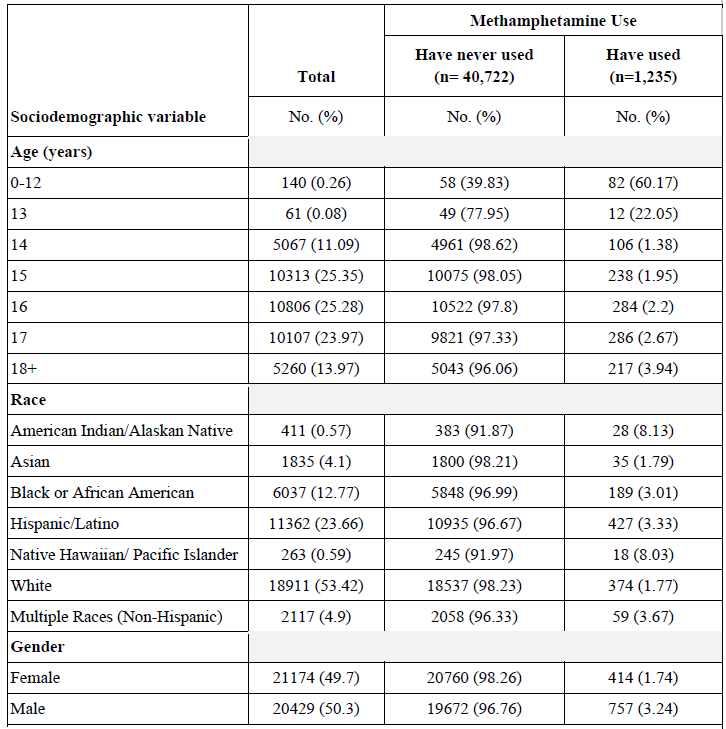
Response rates vary by sociodemographic item inclusion.
Table 2. Prevalence of HIV/STI testing, alcohol or drug use before sexual intercourse, and sexual violence behaviors in adolescents with and without a history of methamphetamine use (n = 1,235)
References
1. Zapata LB, Hillis SD, Marchbanks PA, Curtis KM, Lowry R. Methamphetamine Use Is Independently Associated With Recent Risky Sexual Behaviors and Adolescent Pregnancy. Journal of School Health. 2008;78(12):641-648. doi:10.1111/j.1746-1561.2008.00360.x
2. Baskin-Sommers A, Sommers I. Methamphetamine use and violence among young adults. J Crim Justice. 2006;34(6):661-674.
3. Kelder SH, Perry CL, Klepp KI, Lytle LL. Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. Am J Public Health. 1994;84(7):1121-1126.
4. Lyoo IK, Yoon S, Kim TS, et al. Predisposition to and effects of methamphetamine use on the adolescent brain. Mol Psychiatry. 2015;20(12):1516-1524.
5. Springer AE, Peters RJ, Shegog R, White DL, Kelder SH. Methamphetamine use and sexual risk behaviors in U.S. high school students: findings from a national risk behavior survey. Prev Sci. 2007;8(2):103-113.
6. Taylor-Seehafer M, Rew L. Risky Sexual Behavior Among Adolescent Women. Journal for Specialists in Pediatric Nursing. 2000;5(1):15-25. doi:10.1111/j.1744-6155.2000.tb00082.x
7. National Institute on Drug Abuse. Methamphetamine DrugFacts. Published May 16, 2019. Accessed May 10, 2021. https://www.drugabuse.gov/publications/drugfacts/methamphetamine
8. Shearer RD, Howell BA, Bart G, Winkelman TNA. Substance use patterns and health profiles among US adults who use opioids, methamphetamine, or both, 2015-2018. Drug Alcohol Depend. 2020;214:108162.
9. Kann L, McManus T, Harris WA, et al. Youth Risk Behavior Surveillance - United States, 2015. MMWR Surveill Summ. 2016;65(6):1-174.
10. Rasberry CN, Liddon N, Adkins SH, et al. The Importance of School Staff Referrals and Follow-Up in Connecting High School Students to HIV and STD Testing. J Sch Nurs. 2017;33(2):143-153.
11. Center for Disease Control and Prevention. 2019 YRBS National, State, and District Combined Datasets User’s Guide. Division of Adolescent and School Health, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; 2020. Accessed July 5, 2021. https://www.cdc.gov/healthyyouth/data/yrbs/pdf/2019/2019_YRBS_SADC_Documentation.pdf
12. Youth HIV Statistics & Facts. What Works In Youth HIV. Published August 2018. Accessed May 12, 2021. https://whatworksinyouthhiv.org/youth-hiv/hiv-prevention-treatment/youth-hiv-statistics-and-facts
13. Van Handel M, Kann L, Olsen EO, Dietz P. HIV Testing Among US High School Students and Young Adults. Pediatrics. 2016;137(2):e20152700.
14. Diaz RM. Reasons for Stimulant Use Among Latino Gay Men in San Francisco: A Comparison Between Methamphetamine and Cocaine Users. Journal of Urban Health: Bulletin of the New York Academy of Medicine. 2005;82(1_suppl_1):i71-i78. doi:10.1093/jurban/jti026
15. Semple SJ, Patterson TL, Grant I. Motivations associated with methamphetamine use among HIV men who have sex with men. J Subst Abuse Treat. 2002;22(3):149-156.
16. Semple SJ, Patterson TL, Grant I. The context of sexual risk behavior among heterosexual methamphetamine users. Addict Behav. 2004;29(4):807-810.
17. Howard ED, Wang MQ. Psychosocial correlates of U.S. adolescents who report a history of forced sexual intercourse. J Adolesc Health Care. 2005;36(5):372-379.
18. Yen CF. Relationship between methamphetamine use and risky sexual behavior in adolescents. Kaohsiung J Med Sci. 2004;20(4):160-165.
19. Brewster KL, Tillman KH. Sexual orientation and substance use among adolescents and young adults. Am J Public Health. 2012;102(6):1168-1176.
20. Shrem MT, Halkitis PN. Methamphetamine abuse in the United States: contextual, psychological and sociological considerations. J Health Psychol. 2008;13(5):669-679.
21. Simultaneous use of alcohol with methamphetamine but not ecstasy linked with aggression among young adult stimulant users. Addict Behav. 2017;70:27-34.