Blake Snow, B.S., Oklahoma State University College of Osteopathic Medicine at Cherokee Nation, Office of Medical Student Research, Tahlequah, Oklahoma
Sean Hayes, B.A., Oklahoma State University College of Osteopathic Medicine at Cherokee Nation, Office of Medical Student Research, Tahlequah, Oklahoma
Jamison Williams, D.O., Oklahoma State University Medical Center, Department of Radiology, Tulsa, Oklahoma
Samuel Jellison, D.O., Oklahoma State University Medical Center, Department of Radiology, Tulsa, Oklahoma
Donald Von Borstel, D.O., Oklahoma State University Medical Center, Department of Radiology, Tulsa, Oklahoma
Corresponding Author: Kaylee Mach
kamach@okstate.edu,1111 W 17th St., Tulsa,
OK 74107, Phone: (405) 385-3532
Blake Snow, b.snow949@gmail.com, 1111 17th St, Tulsa, OK 74107
Sean Hayes, seanphayes17@gmail.com, 19500 E Ross St, Tahlequah, OK 74464
Jamison Williams, jamisondwilliams@gmail.com, 744 West 9th Street, Tulsa, OK 74127
Samuel Jellison, samuesj@okstate.edu, 744 West 9th Street, Tulsa, OK 74127
Donald Von Borstel, donaldvonborstel@gmail.com, 744 West 9th Street, Tulsa, OK 74127
Author Contributions: Mach, Snow, and Williams had access to all of the patient demographics and imaging studies in the report and take full responsibility for the integrity of the accuracy of the case. Study concept and design: Williams, Mach. Acquisition, analysis, or interpretation of imaging: Williams and Jellison. Drafting of the manuscript: Mach, Snow, and Hayes. Critical revision of the manuscript for important intellectual content: Williams, Jellison, and Von Borstel.
Ethical Statement: Research conducted through OSU-CHS adheres to the 1979 report of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research, Ethical Principles and Guidelines for the Protection of Human Subjects of Research (“The Belmont Report”). Case reports are not considered to be human subject research under the purview of the IRB (45 CFR 46.104 Exempt Research 4.ii.). Therefore, this case report did not require review by the OSUMC Ethical Committee for the Protection of Human Subjects.
Conflicts of interest/Declarations: The authors declare no conflicts of interest.
Funding: None
Abstract
Non-contrast computed tomography (CT) is the initial imaging modality of choice for acute stroke symptoms.5 Other imaging modalities, such as CT angiogram (CTA) and CT perfusion studies, can help confirm ischemic stroke, identify viable tissue, and determine therapeutic intervention.1 One of the earliest signs of ischemia on non-contrast CT in stroke patients is the hyperdense middle cerebral artery sign (HMCAS).2 The HMCAS is suggestive of acute occlusion within the branches of the middle cerebral artery (MCA).3 In this case, a patient presented with delayed-onset neurological symptoms in the presence of the HMCAS. Imaging proved to guide the therapeutic approach and gave insight necessary to reveal arterial involvement and tissue injury. Identification of this HMCAS in patients is valuable as its presence has been directly correlated to poor clinical outcomes when treatment is delayed.4
Introduction
Non-contrast computed tomography (CT) is the initial imaging modality of choice for acute stroke symptoms.5 This is due to the ability of non-contrast CT to differentiate between hemorrhagic and ischemic stroke.1 In the setting of acute ischemia, one of the earliest markers on non-contrast CT is the hyperdense middle cerebral artery sign (HMCAS).4,6 This hyperdensity is suggestive of thromboemboli within an artery, most commonly the middle cerebral artery (MCA), causing vascular occlusion.3,4 Identification of HMCAS is diagnostically advantageous, expediting the patient towards anticoagulation therapy or surgical intervention. Therefore, the recognition of early manifestations of cerebral ischemia on non-contrast CT is imperative for accurate diagnosis and therapeutic guidance.
Case Report
A 40-year-old female with a past medical history of non-ST elevated myocardial infarction, peripheral artery disease, and deep vein thromboembolism who presented to the emergency room with respiratory distress, nausea, and vomiting. Upon arrival, the patient was unable to follow commands, obtunded, and hypoxic with a room oxygen saturation of 86%. Given the patient's altered mental status, non-contrast CT, CT angiogram, and CT perfusion studies of the head were ordered. Additionally, a breathing treatment was administered due to the patient’s respiratory distress. Imaging revealed high-attenuation of the right middle cerebral artery (MCA) signifying arterial occlusion without intracranial hemorrhage.
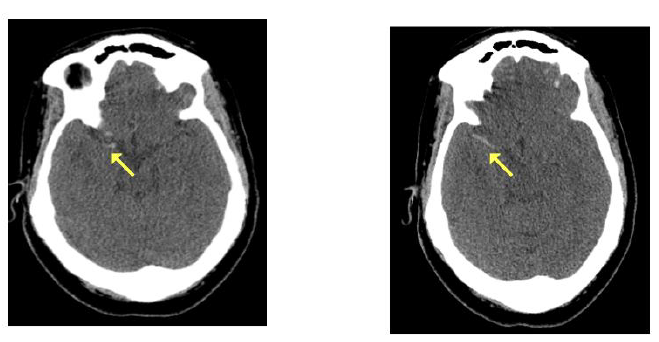
Figure 1: Non-contrast enhanced CT images in the axial plane revealing a hyperdense right MCA indicative of thrombus with vessel occlusion (yellow arrows).

Figure 2: Axial CT angiogram images revealing decreased enhancement of the right. MCA on multiple images consistent with MCA obstruction (red arrows).
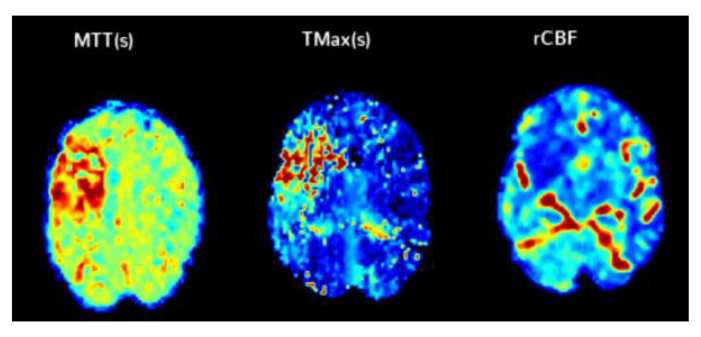

Figure 3: CT perfusion exam with measured mean transit time (MTT) and time to maximum (Tmax) with calculated cerebral blood flow (rCBF). The measured rCBF of 20cc identifies the core infarction, which is the brain tissue that has already been lost to infarction or is expected to be lost regardless of reperfusion therapy. The Tmax of 92cc identifies the infarct penumbra, which predicts the extent of ischemic progression in patients without reperfusion.
Reevaluation of the patient showed new-onset left-sided facial drooping as well as left upper and lower extremity paralysis. Thrombolytics were not administered due to the patient’s symptomatic onset exceeding the therapeutic window at the time of diagnosis. Thrombectomy was deemed a suitable treatment and the patient was transferred for urgent intervention.
Thrombectomy resulted in complete reperfusion of the right MCA with successful stabilization of the patient. Post-procedural CT demonstrated right basal ganglia parenchymal hemorrhagic transformation and effacement of the right anterior horn. Days later, repeat CT revealed stabilization of the basal ganglia hemorrhage with expected evolution. Anticoagulation therapy was held at this time until future neurological clearance.
The patient was routinely extubated and remained stable with minimal residual symptoms. Follow up with neurology was recommended upon discharge.
Discussion
In this study, our patient presented to the emergency room with a history of chronic vascular disease and new-onset neurological symptoms. Subsequent imaging revealed HMCAS on non-contrast CT suggestive of acute ischemia (Figure 1). Additional imaging confirmed a thromboembolic occlusion within the first segment of the right MCA. Due to the significance of MCA involvement, neurosurgery was consulted and an endovascular thrombectomy was performed to initiate MCA reperfusion. Given these results, our findings coincide with poor clinical outcomes and neurologic deterioration in patients with ischemic stroke presenting with a HCMAS.
Along with non-contrast CT, using different imaging modalities like CT angiogram can be useful in identifying the etiology of an occluded artery by allowing visualization of the intracranial blood vessels.6 CTA can also be used to identify the affected brain parenchyma and explore the potential collateralization of blood flow.6 In our patient, the CTA represented a filling defect with the right MCA consistent with our non-contrast CT findings (Figure 2). To assess the viability of brain tissue following an ischemic stroke, a CT Perfusion study was obtained to see the sufficiency of collateral blood flow, in order to delineate injured tissue from salvageable tissue.7 The area identified in red (rCBF of 20cc) represents the core infarct, which is the area considered unrecoverable from infarction. The area identified in green (Tmax 92cc) is the penumbra, known as the area at risk of infarction that can still be recovered with reperfusion. The difference between these two values, the "mismatch", was 72cc. This measurement indicated thrombectomy was valuable to recover salvageable tissue in this patient (Figure 3). By obtaining these additional studies, we were provided insight into specific tissue involvement, allowing for a guided therapeutic approach.7
Another early imaging sign that can be observed on non-contrast CT is loss of insular ribbon presenting as a hypodensity deep within the insular cortex. The insular ribbon becomes the region most distal to perfusion during MCA occlusion, leading to watershed infarction and acute cerebral edema.8 Additionally, loss of gray-white differentiation (GWD) can be apparent in this stage of ischemia and is often seen with localized brain swelling from cytotoxic edema.9,10 Losing GWD has been clinically associated with cerebral ischemia, poor cerebral outcome, and death with worse outcomes predicted by greater GWD loss.11 Early non-contrast CT findings such as the quick identification of hyperdense MCA, loss of insular ribbon, and loss of gray-white differentiation for radiologists or other observers’ sensitivity is ≤67%.12 These findings allow for prompt intervention to minimize the clinical manifestations of ischemic strokes.
After an ischemic stroke is identified, preventing hemorrhagic conversion within the vessel becomes vital to the therapeutic approach. Hemorrhagic conversion occurs whenever a vessel occluded by a thromboembolism is reperfused resulting in the rupturing of blood vessels allowing blood to enter the extravascular space. If left untreated, hemorrhagic conversion occurs at a rate between 18-42%. However, the use of mainstream thrombolytic therapy decreases this rate significantly to 6-8%.13 This resultant hemorrhagic conversion has been implicated with increased mortality, rendering an accurate diagnosis and therapy selection essential to the patient’s survival.13
Conclusion
The presence of the HMCAS on non-contrast CT is specific for acute embolism and shows an increased likelihood of poor clinical outcomes with associated acute neurological deterioration. Moreover, additional studies can be useful in reducing disability by identifying salvageable tissue and initiating reperfusion therapy.14 Due to the increased morbidity and mortality, it is crucial to be aware of early ischemic signs on non-contrast CT to guide therapeutic intervention in patients with HMCAS.
References
1.Campbell BCV, Khatri P. Stroke. Lancet. 2020;396(10244):129-142.
2. Paciaroni M, Agnelli G, Floridi P, et al. Hyperdense middle cerebral and/or internal carotid arteries in acute ischemic stroke: rate, predictive factors and influence on clinical outcome. Cerebrovasc Dis. 2011;32(3):239-245.
3. Barber PA, Demchuk AM, Hudon ME, Pexman JH, Hill MD, Buchan AM. Hyperdense sylvian fissure MCA “dot” sign: A CT marker of acute ischemia. Stroke. 2001;32(1):84-88.
4. Jensen-Kondering U, Riedel C, Jansen O. Hyperdense artery sign on computed tomography in acute ischemic stroke. World J Radiol. 2010;2(9):354-357.
5. Sarikaya B, Provenzale J. Frequency of various brain parenchymal findings of early cerebral ischemia on unenhanced CT scans. Emerg Radiol. 2010;17(5):381-390.
6. Kilburg C, Scott McNally J, de Havenon A, Taussky P, Kalani MYS, Park MS. Advanced imaging in acute ischemic stroke. Neurosurg Focus. 2017;42(4):E10.
7. Zhang XH, Liang HM. Systematic review with network meta-analysis: Diagnostic values of ultrasonography, computed tomography, and magnetic resonance imaging in patients with ischemic stroke. Medicine . 2019;98(30):e16360.
8. Truwit CL, Barkovich AJ, Gean-Marton A, Hibri N, Norman D. Loss of the insular ribbon: another early CT sign of acute middle cerebral artery infarction. Radiology. 1990;176(3):801-806.
9. Kim H, Kim YT, Song ES, et al. Changes in the gray and white matter of patients with ischemic-edematous insults after traumatic brain injury. J Neurosurg. Published online October 1, 2018:1-11.
10. Shirota G, Gonoi W, Ishida M, et al. Brain Swelling and Loss of Gray and White Matter Differentiation in Human Postmortem Cases by Computed Tomography. PLoS One. 2015;10(11):e0143848.
11. Vigneron C, Labeye V, Cour M, et al. Gray Matter-White Matter De-Differentiation on Brain Computed Tomography Predicts Brain Death Occurrence. Transplant Proc. 2016;48(6):1893-1897.
12. Chrzan R, Gleń A, Urbanik A. Hyperdense middle cerebral artery sign as the only radiological manifestation of hyperacute ischemic stroke in computed tomography. Neurol Neurochir Pol. 2017;51(1):33-37.
13. Zubair AS, Sheth KN. Hemorrhagic Conversion of Acute Ischemic Stroke. Neurotherapeutics. 2023;20(3):705-711.
14. Chen Y, Diana F, Mofatteh M, et al. Functional and technical outcomes in acute ischemic stroke patients with hyperdense middle cerebral artery sign treated with endovascular thrombectomy. Front Neurol. 2023;14:1150058.